GLP-1 weight loss injections have changed the way doctors treat obesity, but they also create a new routine that can feel endless. For people who finally hit a stable plateau, the question is simple and personal. “Will I have to take this every week forever?”
A case series from Scripps Clinic in San Diego suggests the answer might be “not always.” In 30 patients who reached a plateau on weekly semaglutide or tirzepatide, many maintained results after spacing injections to about every other week, and some stretched the interval even further.
What the Scripps team followed in real patients
This was not a large trial designed to set new guidelines. It was a retrospective case series that looked at adults treated at one clinic who transitioned to reduced-frequency dosing at the same dose they had been using.
The analysis focused on 30 patients who stayed on the reduced schedule, while four people returned to weekly injections after gaining weight before the first follow-up visit. Average time on the reduced-frequency plan was about 36 weeks, with a range that stretched from roughly three months to more than two years.
So what did “reduced frequency” mean in practice? Most people reported injections spaced at least two weeks apart, the longest interval reported was six weeks, and a smaller subset fell between 10 and 14 days.
The weight and health markers that held up
On average, patients started around 193.8 pounds before GLP-1 therapy and reached about 163.4 pounds at their weekly-dosing plateau. During the maintenance phase with fewer injections, average weight dipped a bit more to roughly 159.6 pounds.
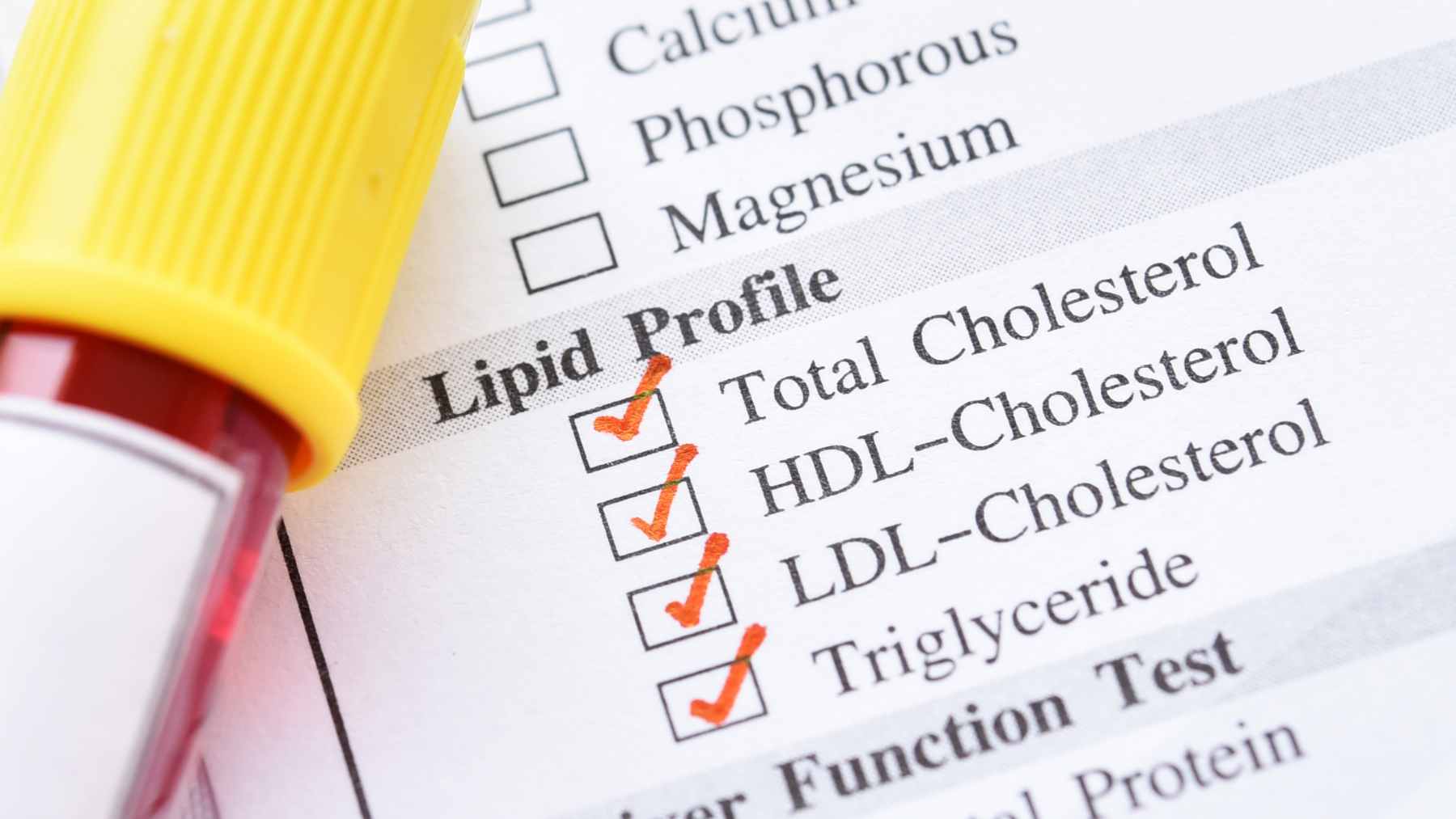
The study also tracked metabolic markers tied to long-term risk. HbA1c, triglycerides, blood pressure, and HDL cholesterol improved during weekly treatment and were largely maintained after the switch to reduced-frequency dosing.
Body composition data came from a smaller subset, but the trend was reassuring. The researchers reported continued small declines in body fat during the reduced-frequency phase, while muscle mass trended toward stability and even a slight rebound.
Why stopping the drug often leads to rebound
The interest in spacing doses is partly driven by what happens when people quit cold turkey. A 2026 Oxford-led systematic review and meta-analysis reported that weight tends to rise after weight management drugs are stopped, and the rebound after newer GLP-1 medicines was faster than after older agents.
In that analysis, regain after newer medicines such as semaglutide and tirzepatide averaged about 1.8 pounds per month, with projections suggesting many people could return close to their starting weight within about a year and a half. Cardiometabolic improvements also tended to drift back toward baseline over time.
A separate 2026 modeling study, built from randomized trial data, estimated that people regained about 60 percent of their lost weight by one year after discontinuation, with regain slowing later and potentially leveling off short of a full return to baseline. That is a different story from “spacing doses under supervision.”
What “structured de-escalation” is and what it is not
The authors described reduced-frequency maintenance as “structured de-escalation” that could reduce treatment burden without sacrificing key outcomes, at least in selected patients. They were also clear that larger randomized controlled trials are needed before anyone treats this like standard care.
It is also not the same thing as “microdosing,” a practice pushed by some influencers that involves taking less than the prescribed amount. Scripps noted their study looked at keeping the same dose while changing the interval, and emphasized that all medications should be taken as prescribed and in line with FDA guidance.
There is a human factor that matters here, too. People who successfully de-escalate may also be more motivated to tighten habits and keep up with follow-up visits, which can skew results in a small observational study.
If you are thinking about stretching doses, here is the safest frame
Start with a clinician-led plan, not a DIY change to your reminder app. FDA labeling for these injections is built around once-weekly dosing, so any change in frequency should be weighed against your full medical history and goals.
Also keep the study’s context in mind. Patients had already reached a plateau and were monitored, and some people did need to return to weekly injections when weight started to climb. That early course-correction is part of the story.
Finally, habits still do real work during maintenance. Strategies that protect muscle, such as resistance training, along with routines that support appetite control and sleep, can help when medication support is dialed down.
The maintenance phase is becoming the next frontier
The Scripps findings land in a moment when obesity care is shifting from the sprint to the long middle mile. When a treatment becomes a years-long habit, the burden is not just medical, it is practical and financial, too.
Researchers are also exploring other ways to make maintenance easier. In May 2026, Eli Lilly reported trial results suggesting an investigational oral GLP-1 pill called orforglipron helped many people maintain a large share of their weight loss after transitioning off injections, compared with placebo.
For now, the most responsible takeaway is modest but meaningful. “Less frequent” may be possible for some people after a plateau, but it is not a shortcut, and it is not yet a guideline.
The study was published on Obesity.