Menopause is often treated as the day periods stop. In reality, the body may begin changing years earlier, with shifting hormones affecting sleep, bleeding, sexual health, concentration, and mood.
That longer transition is the focus of a recent Brazilian podcast discussion with specialists in gynecology and psychiatry. Their message is simple: symptoms can start around age 40, vary widely, and do not have to be silently endured.
The transition starts before the final period
The ‘climacteric’ is the broader shift from the reproductive years into life after menopause. ‘Perimenopause’ is the part when periods and symptoms begin to change, while menopause is confirmed only after 12 consecutive months without a period and no other clear cause.
The podcast specialists said the climacteric can begin seven to ten years before the last menstrual period, with discomfort sometimes appearing around ages 40 to 42. Timing is personal, though. The World Health Organization says most natural menopause happens between ages 45 and 55 worldwide.
Why hormones feel unpredictable
Why can someone still menstruate and already feel very different? During perimenopause, the ovaries become less consistent at releasing eggs and producing estrogen, so hormone levels can rise and fall rather than decline in a straight line.
That instability can change cycle length and flow, making periods closer together, farther apart, lighter, or heavier. Estrogen also affects temperature control, vaginal and urinary tissues, bone, and the cardiovascular system. That is why the experience reaches far beyond a missed period.

A woman experiences a hot flash while working, one of the most common symptoms of perimenopause and menopause. Doctors say hormonal changes can also affect sleep, mood, memory, and concentration.
Hot flashes are only one part
Hot flashes and night sweats are the best-known symptoms, and the U.S. Office on Women’s Health says as many as three in four women experience hot flashes. A sudden wave of heat can interrupt a work meeting, a commute, or a full night’s sleep, then disappear just as quickly.
Other changes may include insomnia, joint discomfort, headaches, palpitations, fatigue, and shifts in body composition. Not every symptom comes from menopause, so a medical review may be needed to check for other causes.
Lower estrogen can also make vaginal tissue thinner and drier, causing burning, painful sex, or urinary symptoms. These problems often go unmentioned, even though treatment is available.
The mind can change, too
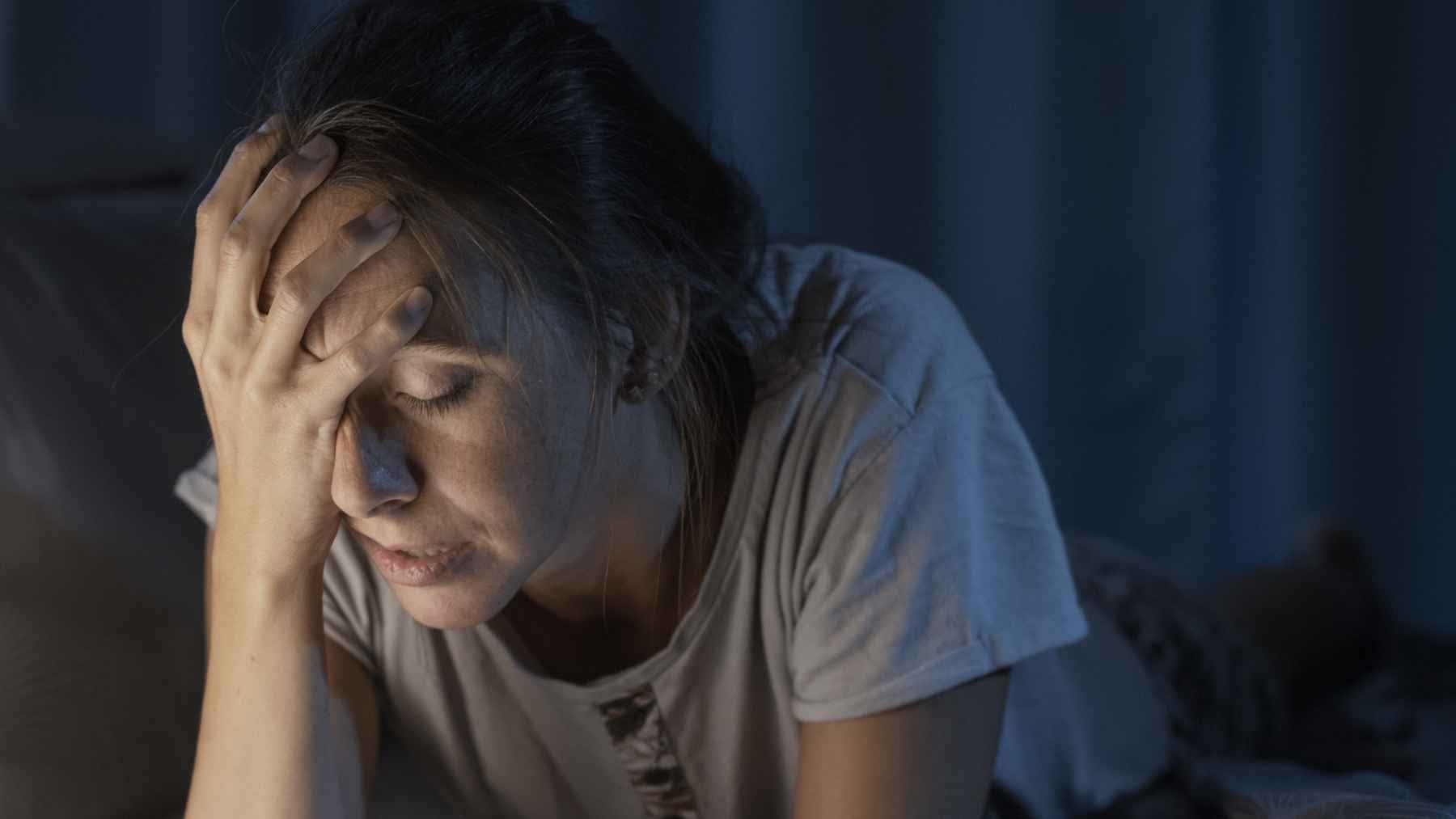
Irritability, anxiety, low mood, forgetfulness, and trouble concentrating may appear during the transition. The familiar label is “brain fog,” but it can feel very real when names, tasks, or words suddenly seem harder to retrieve.
The American College of Obstetricians and Gynecologists says about four in ten women report mood symptoms during perimenopause that resemble premenstrual syndrome. Hormone swings may play a role, but broken sleep, hot flashes, work pressure, caregiving, and previous mental health conditions can pile on.
Depression is not inevitable. Still, research has found a higher risk of significant depressive symptoms during perimenopause, particularly alongside hot flashes or stressful life events. Persistent sadness, panic, or loss of daily function deserves professional attention.
No two women follow the same script
Some women notice only irregular periods. Others have symptoms for years that affect relationships, work, exercise, and ordinary routines. That wide range is why one-size-fits-all advice often falls short.
Culture and access to care also shape the experience. When menopause is treated as embarrassing or simply something to endure, women may not connect their sleep, mood, or sexual symptoms to the transition, delaying help.
Treatment should fit the person
Tracking bleeding, hot flashes, sleep, mood, and medications can help reveal patterns. Bleeding changes are common, but very heavy bleeding, bleeding between periods, or any bleeding after menopause should be evaluated.
For troublesome hot flashes and night sweats, hormone therapy remains the most effective treatment, according to The Menopause Society, but it is not right for everyone. Age, time since menopause, medical history, preferences, and individual risks all matter.
Nonhormonal medicines may reduce hot flashes, while moisturizers, lubricants, or low-dose vaginal estrogen can help dryness and pain. Counseling, psychotherapy, and psychiatric treatment can address anxiety or depression. In other words, care may involve more than one professional.
Long-term health still matters
After menopause, lower estrogen is linked with faster bone loss and changing cardiovascular risk. Weight-bearing exercise, a balanced diet, not smoking, and routine health checks can support healthy aging.
Pregnancy can still occur during perimenopause, so contraception may be needed until menopause is confirmed. Menopause is not a disease, it is a life stage that is easier to manage when symptoms are named early and taken seriously.
A conversation across specialties
Host Camila Oliveira explored the subject with gynecologist Camila Rabello of Angiclin Clinic and psychiatrist Luciana Oliva of Holiste Psychiatry Clinic. Rabello studied medicine at the Federal University of Bahia, while Oliva completed psychiatry residency there, bringing physical and mental health into one conversation.
That combined view is the episode’s strongest point. A hot flash, a restless night, and a wave of anxiety may look separate, but during this transition they can be connected.
Recognizing the pattern earlier can turn years of confusion into a clearer plan for care.
The official episode was published by Globo Podcasts.